 Live Music Archive
Live Music Archive Librivox Free Audio
Librivox Free Audio Metropolitan Museum
Metropolitan Museum Cleveland Museum of Art
Cleveland Museum of Art Internet Arcade
Internet Arcade Console Living Room
Console Living Room Books to Borrow
Books to Borrow Open Library
Open Library TV News
TV News Understanding 9/11
Understanding 9/11tv Charlie Rose PBS December 17, 2012 12:00pm-1:00pm EST
12:00 pm

parent. and that was especially true today. i know there's not a parent in america who doesn't feel the same overwhelming grief that i do. the majority of those who died today were children. beautiful little kids between the ages of five an ten years old. they had their entire lives ahead of them. birthdays, graduations, weddings, kids of their own. among the fallen were also teachers, men and women without devoted their lives to helping our children fulfill their dreams. so our hearts are broken
12:01 pm

today. for the parents and grandparents, sisters and brothers of these little children, and for the families of the adults who were lost. our hearts are broken for the parents of the survivors as well. for as blessed as they are to have their children home tonight, they know that their children's innocence has been torn away from them too early. and there are no words that will ease their pain. as a country we have been through this too many times. whether it's in elementary school in newton or a shopping mall in oregon or a temp el in wisconsin, or a movie these never aurora or a street corner in chicago, these neighborhoods are our neighborhoods. and these children are our children. and we're going have to come together and take meaningful action to prevent more tragedies like this regardless of the politics.
12:02 pm

this evening michelle and i will do what i know every parent in america will do, which is have our hold our children a little tighter and we'll tell them that we love them. and we'll remind each other how deeply we love one another but there are families in connecticut who cannot do that tonight. and they need all of us right now. in the hard days to come that community needs us to be at our best as americans, and i will do everything in my power as president to help. because while nothing can fill the space of a lost child or loved one, all of us can extend a hand to those in need, to remind them that we are there for them, that we are praying for them, and that the love they felt for those they lost endures not just in their memory-- memories but also in ours.
12:03 pm

may god bless the memory of the victims. and in the words of scripture, heal the broken hearted, and bind up their wounds. >> rose: flags at the white house and the capitol are flying at half-mast in recognition of one of the worst school shootings in american history. the victims and their families are in our thoughts and prayers this evening as we air a program on a brain series about post traumatic stress disorder. after this break, our program on post traumatic disorder begins. funding for charlie rose was provided by the following:

12:05 pm

from our studios in new york city, this is charlie rose. it is estimated that one in five american veterans in these wars suffer from severe depression or post traumatic stress disorder. retired lieutenant colonel john o blin is one of them. he served four tours in iraq and surrounding persian gulf as well as three tours on the-- tours on the border of israel and egypt, awarded the bronze star, purple heart and kbrat action badge among other commendationses. he joins me tonight to talk about his life, also joining me an extraordinary group of scien titss, mary stein from california san diego, lisa shin from tufts university, kerry russler from emory university, joann difede from cornell and my cohost is dr. eric kandel. a noubl lawyer yet, professor at columbia university and a howard hughes medical investigator. i am pleased to have all of them here this evening at this table.
12:06 pm

which begin as we always do talking to eric kandel. what are we doing this evening. >> post traumatic stress disorder. this is a fascinating disorder. and it is unique in psychiatry. it is perhaps the only psychiatric disorder whose cause we really understand well. post traumatic stress disorder is a response to the physical threats to the integrity of one's self or someone else. it is associated with feeling of tremendous fear and helplessness. we are privileged to have john o'brien with us today who can tell us directly what it's like to experience post traumatic stress disorder. as you pointed out he's an american hero. he just retired from being lieutenant colonel in the army. and served 25 years of duty including service in iraq where he first developed post traumatic stress disorder. post traumatic stress disorder as you pointed out is no rare-- to the rare,
12:07 pm

it's also not a recent disorder, estimate its range from 15 to 25% of troops coming back from this current war suffer from post traumatic stress disorder. moreover although it's only been recognized at a specific diagnostic category for about the last 30 years, post traumatic stress disorder has been with us since people have been going to battle. the trojan war one of the arearl wsts on w record, e heromer skroobed in the iliad took placeroyblbaro 00 bc and homer wrote t it inab 8,000 bc. there he describes how achillesib rrurte hlyt ht by the death of hisosestt friend by hector thead leer of the trojan tr a rampage in which h a raage in which he arsttod a ill people, und hector, killed him, screaming nothing matters to me now but killing, blood, and men ining aonee. tied after to his chariot and dragged him around the
12:08 pm

grave three times. and homer points out that you not only suffer from post traumatic stress disorder, which is not the name he used, you suffer from this disorder if you are a victim of violence but also a perpetrator of violence. an in fact, achilles releted-- repeatedly had reminisces of this and bad dreams about this afterwards. american troops have been suffering from post traumatic stress disorder since america existed, in the war of independence, in the civil war, world war i, world war 23, all the subsequent wars. but it wasn't until the aftermath of the vietnam war because of the, you know, political unpopularity of the war that this was considered a serious diagnostic category. in 1980 the american psychiatric association officially designated it that. but in the early days, because the evidence of post traumatic stress disorder comes from an individual
12:09 pm

report, people were skeptical about the reliability of its, thought this was a way of soldiers found to avoid going back to the front. they called this bad behavior and as "the new york times", which by the way seems to be calling our programs each time, last time they did pain, now they are dos post traumatic stress disorder, they must be watching what is happening on charlie rose. >> rose: they could do worse. >> they could do a lot worse. (laughter) >> so they pointed out that veterans from the vietnam war suffer a double hurt. first of all they have the disease, the post traumatic stress disorder but in addition because many of them were thought to be malingerers, bad behavior they did not get an honorable discharge. this is no longer the case. this is now considered a legitimate category and people who suffer from it are treated appropriately. and one of the reasons it is a legitimate category is because in addition to having a good clinical
12:10 pm

definition we are beginning to have some biological markers of it. we know a little bit about the genetics. so we know from imaging experiments this of what we will discuss here that there are three areas in particular that are involved in post traumatic stress disorder. the a mig delia, the prefrontal cortex which regulates the amigdila and the hypocampus. and hypocampus is shut off in part by post traumatic stress disorder. and that is thought to account for some of the misplacements of memory and distortions of memory that occurs. also there is evidence for genetic participation in this. if you have an identical twin that has post traumatic stress disorder the likelihood of you getting post traumatic stress disorder is much greater than if you had a twin who is not identical. post traumatic stress disorder doesn't simply occur as a result of war. it also occurs in civilian life. and interestingly there
12:11 pm

women are much more susceptible to post traumatic stress disorder than men, because they are more susceptible to sexual abuse, physical violence. but in addition to just physical brutality there are other things that can contribute to post traumatic stress disorder. natural disasters, things like 9/11, hurricanes and storms can all-- particularly if people are in awkward situation relationship can trigger post traumatic stress disorder. the symptoms of post traumatic stress disorder in addition to helplessness have other features. nightmares, recurrent bad ideas, bad frightening thoughts, a tendency to avoid the situation that in any way recalls it. so this is really a very painful experience. although we have only considered this as a diagnostic category for 30 years, it's amazing how much we know about the biology of this. charles darwin realized that we convey emotions through
12:12 pm

our faces. and was very much interested in the expression of emotion. and he pointed out that emotions are amazingly conserved among different people. if u are going to llop arleveh o t ie world, they express tham see six or seven proto tipic emotions and expressive of theeam s facial features so you see, for ex ple,ssar esdn in the leftndes apiapne hss in the right. and this is prettyss universal. not only tt,hay he realized profoundly thatis h evolutionary conservednis a ale animals this was mpcompleanimal, o rag n t even mend a a rats show ymotional responseser v milar to that of humans, an darwin chose this picre of a human beingnd a o rang a tan showing a very similar response. to emotion. and the reason this is so power sfl that many people have been influenced by darwin's realization about the conservation of behavior and emotional response and used simple animals as we're going to hear about this afternoon, to study post
12:13 pm

traumatic stress disorder which we can produce rather readily in mise and in rat its. there we can learn about the genetics of it, about the neurosystems that are involved and a masesingly we can also get some insights into treatments that could reverse it in animals that can then be applied to people. so we're going to hear a number of different approaches to trying to help people with post traumatic stress disorders. psycho therapy groups as well at things that have come, farmco therapy that have come out of animals. so this is really a remarkable disorder in which not only do we have a very good understanding of what causes it but we're beginning to get some insight into how to treat it. so we're in for a very exciting discussion. because these are the people that have pioneered it and john is the person who has experienced it. >> rose: let me turn to mary stein,-- murray stein, give me an overnight adding to what eric said and the prevalence of it. >> so as dr. kandel mentioned post traumatic
12:14 pm

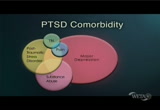
stress disorder is very common in our military personnel who have been returning from iraq and afghanistan, and the rates, you heard, are up to one in five people with post traumatic stress disorder or depreltion, substance abuse, those all kind of travel together. but it's also very common in civilian life so in the u.s. general population, estimates of similar around 2 to 3% of people have post traumatic stress disorder in their lifetime. some people are more likely to develop ptsd because of their occupations. a lot of post traumatic stress disorder in firefighters, in policemen and women. and then as eric also mentioned, more ptsd in the general population in women than in men in large part because of the kinds of traumatic experiences women are often exposed to, domestic violence, sexual trauma and the like. >> rose: is the core here the fear, whether it's from war or from civilian life, the idea of the constant
12:15 pm

fear of being assaulted? >> so the core is really that something life threatening has happened to profoundly change the individual's view of the world and their expectations. and a big part of it then is this ongoing fear that it could recur, it could happen again, it's going to come back opinions when did you first notice it, john. when did you become aware that what you had been experiencing might be something not-- what everybody experiences. >> it doesn't suddenly happen. and i think after doing, you know, the four deployments over to that part of the world, it kind of cent up on me slowly. i first noticed maybe i was on leave, in fact. and i was in a hotel and i woke up in the corridor of the hot well no idea how i got there i was sleep walking. and i kind of put that aside. and tried to let that go. and then nightmares started to creep in. and i noticed when i kept going back after leave or another deployment, it was great. i was fine over there and i
12:16 pm

would come home. and that's when i would start to get sad. i would cry for no apparent reason. i isolated myself. and i would just stay in my apartment. and not go out. and then ultimately the symptoms did get worse to incredible boughts of and-- bouts of anger, for no apparent reason just getting extremely frustrated, even yelling out my apartment window because the fire trucks were too loud. and so it was an incredible-- . >> rose: what did you think was happening? >> i did not want to think it was ptsd. i grew up-- . >> rose: which you were familiar. >> oh, yes, absolutely. but it's always, it's the men. you got to worry about them. it's going to happen to them. it's not going to happen to you. i'm a senior officer. it can't happen to me. so i had been in long enough to know that this wasn't going to happen to mement and sure enough it did. and it didn't just go away. it didn't get better, it got worse. and i realized that i had to
12:17 pm

get out of new york city. it was too much stimulation all the time. and so i did. i moved and i moved to an island off the coast of rhode island. and that took some adjustment as well. >> i'll bet. >> rose: but prior to doing that and realizing the things that i needed to go to help, i went through the dod study that i think you could explain better as far as that medicine goes, this type of psychotherapy that helped me, incredibly. it doesn't get rid of ptsd. it helps you deal with it better, think about it more logically, process it better. and i think those tools that you learn in this program plus maybe that medication. >> do you think you could explain to us a little bit about how your life has changed with therapy and what's different? >> well, now i recognize that, yes, i do have ptsd.
12:18 pm

and i'm not embarrassed about it any longer. but it caused me to think about these things that happen. for example, not just a horrifying event that took place but it was bizarre. and that was in the republican balance as in baghdad. i was there for a meeting with the force protection colonel. and of course as usual the rockets come in. and they're blowing up outside. and then i see smoke coming from down the hallway, a lot of smoke. and we were running down. we go in. and as soon as i enter the room i see where the smoke is coming from. it's coming from the engine of a rocket, but still it's embedded in the floor of the wall and i'm like wow, that's-- and so i went further in the room to see if anybody was in there. and sure enough there were. there were two people who were dead and one woman, she was a civilian, she was literally cut in half by the rocket. and the lieutenant commander basically had his face taken
12:19 pm

off. and it, these are images and the smell too, the caustic odor of the rocket propellant, i can still sense it talking about it. and i can see those images. and i-- and right now, you know, my heart's racing now. >> rose: as you speak. >> as i'm speaking because, you know, i thought for sure the rocket was going to blow up. >> what is interesting and i gather very common is that particularly people in responsibility are reluctant to admit to themselves that they're suffering from post traumatic stress disorder. and here as in all other medical disorders the earlier you get treatment, the easier it is for you to recover. how long did you wait before you started to seek treatment of any sort? >> i was ordered by the army to go during-- well, i came back and -- >> and it was part of the
12:20 pm

medical evaluation board process. i had had a heart attack and had four stents put in my heart. and when i came back the last time, i was in the airport and it was the classic heart attack, the crushing chest pain, sweating, nausea, pain in the arm and shortness of breath. and that caused the army to send me through an incredible physical evaluation. >> well, i can understand. >> and a lot of that changed me too, and i they were able to push the right buttons. but even before that i was told or recommended when i came back after i think it was in 2005, i went through the line, the outprocessing line and saw a psychiatrist. and she pressed the right button. she said you should probably see stb afterwards. you probably have post traumatic stress disorder. >> rose: were you surprised? >> yes, i was. i said i come from a city of 8 million people with ptsd.
12:21 pm

and she said excowes me. i said, well, remember 9/11, yeah, you know, i watched the second plane hit. and how many other people, how many people lost loved ones there, very horrifying. and so maybe that was the beginning. but again, i couldn't bring myself to, you know, here i was a lieutenant colonel, you know, i'm in the infant ree a signed to special operations command. and it was-- it is not easy to admit. it is embarrassing at first, i think. >> rose: tell me about imaging and what we're learning? >>. >> well, in the last 20 or 30 years imaging in medical science has advance advanced to the degree so that we can actually use techniques like functional magnetic resonance centre imaging or fmri and pet scanning to actually take pictures of the activity in the human brain. and we can do this noninvasively. so the visual is showing you fmri machine right now. and so if we're interested
12:22 pm

in understanding the brain mechanisms underlyingtsd, we could hvea people withve ptsd in the scanner recalling their own traumatic events and neutral events as well. we could also show them their queues or triggers. or we could show them emotional material and then observe the activity of the brain. and actually researchers have been doing this for the past 20 years to study ptsd. and they've largely focused on a couple different brain-- well, several different brain regions but i will talk about a couple of them. the first is the a mig da labs, the temp ral lobe structure, one on the right and left. and the it is responsible to threat or po tleningts in the environment. so this is the a good thing. we want the amidala to do this for us because we want to prepare for the threat. we want to either fight or run away or find out more about that potential threat in the environment. but sometimes the amigdala
12:23 pm

may get it wrong so it may respond too strongly or in times when it's not needed. and we think this might be what is happening in anxiety disorders including post traumatic stress disorder. so the visual on the right is showing activation that's greater in the right amigdala in individuals with post traumatic stress disorder compared to trauma exposed individuals without ptsd. and it turns out in that one study, anyway, and actually several studies the greater the ptsd, the greater the amigdala activation. but there is also another part of the story. and that is medial prefrontal cortex. and that is another brain areas that's actually right in the middle of the two hemispheres of the brain in the front of the brain as shown in the visual this is an area that we think inhibits the amigdala involved in regular lalingt-- regulating emotion, and learning and remembering that something that used to predict threat
12:24 pm
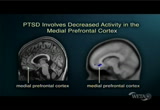
actually now no longer does and that process is called extinction and you need a medial prefrontal cortex in fact to occur normally. this is an area of the brain that we think is under or hyporesponsive in individuals with ptsd as shown in the visual. the blue area is showing less act valtion in people with ptsd compared to trauma exposed individual was ptsd. and the greater the symptoms severity the let's the activation there. and we think that less activation in this region may underlie some of the problems with emotion regulation. and also the difficulty disengaginging from trauma related cues or triggers. >> and probably protective factors may come from being able to recruit that very effectively. >> correct. >> rose: let me turn to kerry and tell wlaus is going on. >> what is interesting about the area of fear is that although on the one hand it is out of control with the hypersensitivity in the fear response in ptsd and phobia
12:25 pm

and panic but it is evolutionarily useful. and mammalian species from mice to men share the same bake processes. what we see say fearful cue like a snake figure projected on to the retina, and that visual information is passed to the first weigh station in the brain, the thalamus passed on to the higher order visual cortex. that interprets what this image is that we are are seeing. >> rose: friend or foe. >> exactly. and both this information from the thalamus and cortex are send to the amigdala and that is the weigh station that says is this bad memory or not and activates the fight or flight system, the freezing response, blood pressure response, auto nomic response. what is particularly interesting about this area is again that it is so conservative-- across animals. so we study this mostly using a technique called classical conditioning that was first described by pavlov in st. petersburg, rush ab, over 100 years, most people are familiar with pavlov dog with the repetitive condition, the bell, the food, it turns out
12:26 pm
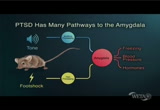
a lesser known component as well as fear kong, the same bell with pain or foot shock would lead to dogs with fearful behavior. we did this daily across the world in rodent studies and mice we can study the genetics and nearal systems that mediate this process. and in this visual in a typical mouse study you have a sound or tone activated the auditory parts of the brain, the foot shock at the end of the tone, the pain parts. they come together in the amigdala where this memory is formed so in future times when the tone is played it activates the same freezing. >> just from the tone. >> just from the tone. >> sometimes patients say it feels like those memories are indelibly in, and it is as if you are reliving it. we have a video to show what this look like when we train a mouse. both of these mice have been handled before. the one on the rite has been trained to be afraid of the cue. the one on the left has not heard the cue. when the tone comes on we'll find the one on the right reoriented and then freezes
12:27 pm

and pretty much freeze for the remainder of the 30 seconds while the other continues to explore. we're doing this in red boxes because piece are nocturnal and tend to show more basal behavior in the dark. >> rose: what is that. >> their normal curious walking around, exploring so we can tell the one on the left is continuing to move and the one on the right is totally frozen. >> just terror. you can tell how that is protecting him from the hawk or snake that is to the going to see him because he is not moving. as soon as the tone goes off he starts walking around again. >> another interesting thing it is a little like pain, pain is a protective modality but when it becomes excessive it becomes a disease state. so is fear response, a normal part of living. we want to escape things that are dangerous but when it becomes overactive. >> rose: that happened with the nightmares, i remember that clearly. and that's what interested me in that video when i first saw it was when you wake up from it, you are freeze, you don't move, are you afraid to move. any movement could get you killed, maybe. who knows.
12:28 pm

>> i would never mistake you for a house though. >> if we take this idea of the amigdala and expand it beyond this basic fear, but you tacked about the blood pressure that you experienced simply talking about the story, how the sweating, the stress hormone response, upset stomach, the freezing you can even experience as a human, the startle response. these are all hard wired reflexes of the amigdala. what is fascinating is the psychology field has identify these as the hard wired fear reflex. whereas the clinical world found these as the basic symptom clusters of ptsd, panic disorder and phobias. so we think the fear disorders together. and my final slide will get to where we want to go which is how do we understand treatment and prevention. after the fear, trauma occurs this memory is con tme dated. it means it becomes permanent. what we would really like to do is provide a pharmacological or psychological intervention at the time of the trauma to prevent it from overcoming n light of that, people who already have chronic symptoms there seems to be two process that differentiate those with it and those who recover.
12:29 pm
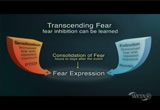
those who get it tend to get sense phized. every time they have the nightmare, it keeps getting worse. alternatively this concept of extinction. pavlov defined extinction as repeated exposure to the cues. we keep ringing the bell over and over and the animal won't be afraid any more that is what we do with exposures therapy. to help improve exposure therapy. >> rose: are you doing a test with john involved in terms of -- >> john actually completed one of our department of defence funded clinical trials current thinking about ptsd is it is a disorder 6 emotion 58 learning and as-- emotional learning. >> so fear conditioning as kerry just described. and so we think whether you are human or a house, fear conditioning or classical conditioning is the underlying model for fear itnditioning. and as you can see in this slide humans en they undergo trauma encode sense ory elements of their cuesience which become of their fear or reminders
12:30 pm

of their experiencso itt used to be prior to 9/11 you could walk down thers yoaist and assume it was a preaiy neutral place but these are people walking down a simulated stairwell of the world trade center attack. and after 9/11 it was no longer safe to assume that people were, would feel neutral to a stairwell. we have patients who quite their jobs because they couldn't walk up the stairs. they couldn't take the elevator up to the 30th floor norwalk down the stairs any longer. so that is both an example of conditioned fear, with the cue being the stairwell. and avoid anlts because the person quit their job. now in exposure therapy which is the type of treatment that john receives in our clinical trial, patients recount their experience whatever their specific traumatic event was, whether it is a particular event that john had in iraq or survival of the world trade center which john also personed. >> what do we do now that we know we've got post traumatic stress disorder. >> sure. so it turns out that you know we've talked about ptsd
12:31 pm

in sort of the core symptoms in humans, it's actually very complex. not only do people have the sy ptoms but they develop ways of trying to cope with the symptoms. a lot of times as you mentioned both when people develop ptsd to give an example in the military. when people do things as part of their job that they are supposed to do, kill people, hurt people, and they come back into civilian life and they feel tremendously guilty about that or there may be guilt about having survived in a situation where other people didn't. those aren't things we easily model with animal models. so i humans it's much more complex. and we also know and dr. kandel eluded to this that people will use a lot of different substance, develop substance problems to cope with the ptsd. people if they've had a physical injury can have pain symptoms that serve as a reminder of their post traumatic stress disordeir and also develop chronic pain symptoms afterward.
12:32 pm
a lot of people become detres-- depressed so when we're talking about treatment, it's often not simple. but we have some very good treatments out there. joann has talked about expose heuer therapy, prolonged exposure is one that is evidence-based, been show in many studies to work there are others like that. so very good psycho therapies out there. we have a couple of fda approved medications to treat post traumatic stress disorder. these are anti-depressant class medicines which help both with the depression and also with the post traumatic stress disorder and a lot of new developments in trying to find better ways to bring together pharm couldtherapy, so there are a lot of interesting advances that will be coming yen line we hope. >> take it from there. i mean what are we looking at down the road in terms of treatment options? >> well, one treatment option that is included in our department of defence study is an enhancement of this evidence-based treatment, exposure therapy called virtual reality-based exposure therapy.
12:33 pm

and the thinking behind that is that we experience the world in multisensoree dimensions, not just cognitive and verbal encoding. we hear, we see, we smell, we feel our experiences. the virtual reality form of exposure therapy allows for an enhancement of the person's traumatic memory in these different sensoree dimensions. if i request have the video we will see a clip here of it a man whose one of the operations department in the fire department at the time of the world trade center. he's also a naval pilot, by the way. and he wasn't doing well with his traditional treatment. and so we offered. he was actually one. very first persons to receive the virtual reality exposure therapy. >> comfortable. >> yes. >> you can hear me. >> yes. >> stephen king was there the day to the we ares fell. and he's been dealing with it ever since. >> i had a, just such a
12:34 pm

total feeling that i wasn't the same person. >> like many other rescue workers king has post traumatic stress disorder. he's been through therapy but it didn't work. so now he's trying this virtual therapy. >> i was almost shaking. i mean it brought it back like i was there again watching it. >> it's called virtual reality therapy or vrt. and it uses sounds and 3 d images to force patients to face their fears. >> very slowly patients are taken back to their traumatic experiences. and steven's case, a virtual journey back to september 11th. >> here's how it works. first the patient sees the towers as they were before the attacks. then a plane appears and flies behind to the percent. experts say this readies the patient for what is about to happen. next a plane hits the first tower but without sound. then the full experience
12:35 pm

authentic pictures and surrounds taken from video shot that dayment because it is so overwhelming it can take up to 8 weeks for a patient to see this, start to finish. >> if allows us to take it in small steps instead of biting off more than a person can chew in therapy. >> researchers say all those who have gone through vrt have responded well. the new york city fire department says it's familiar with the therapy and has even referred patients to the program. as for steven, he says he's got his life back. >> it really forced me to think about it. and to talk about it. and in opening up that, maybe to understand myself. >> by going back in time to move ahead. >> this is one of the key elements of all psychotherapeutic process. one relives the experience in a protected environment, with a therapist. one is comfortable with and one trusts, so one element is just the safety of being with somebody who listens to you, doesn't pass any
12:36 pm
judgement and just accepts you the way they are. there are many other components but the fundamental component is, would be called transference, a trusting relationship with another persons. >> and that's what we refer to as a safe environment, but over an above that this particular individual's case, we would come in and he would be talking to me as if he was reading the front page of the "new york times". he was numb. he was avoid ant. he had difficulty going over bridges. we have panic attacks but then the second time de the virtual reality exposure, actually the first time he said to me, he said he started pointing out, he was a pie lot. he started pointing out all of the engineering problems with the virtual world. now remember this was an sperm. so i thought to myself oh my goodness maybe we made a mistake. but then the second or third time he came in he saw a building and all of a sudden he said you know what, i just remembered something. and he began to recouldn't an experience in which he heard an fbi agent say, as this man was running down
12:37 pm

the street there is a third plane coming in. what he said to me was my naval training kicked in and i thought when i heard this third plane coming in that we must really be at war and this was not a discreet terrorist incident that that i was going to survive. suddenly i, my chest, i start to feel tight in my chest and i started to panic. he had a panic attack. that was when he had the experience that his life was in danger. but what called it to mind after weeks of talking to me as if he was reading "the new york times" was seeing something that reminded him so it was a visual cue to his experience that allowed him to emotionally engage. and that's one of the reasons why we think the virtual reality form of exposure therapy are working hypothesis is that it may be better for some patients, particularly for parents who are avoid ant and numb so we actually have, we developed a virtual world for soldiers and warriors who are returning from iraq and afghanistan and we have a clip of that if you would like to see it. >> engage. >> i'm engaging.
12:38 pm

>> he's wounded. second one. roger. >> virtual environments were built with a lot of feedback from our warriors. in fact one of the team of people developers actually was a captain, a skol gist in the army. we've got a great shot of him with a laptop on the back of a truck and soldiers in yuchl going up and put on the head mounted display and testing the world and giving feedback as to how to improve it. in the situation we just saw was a situation very common. soldiers are on patrol in a small town and then an ied goes off. and the police come running. for someone like john's
12:39 pm

experience or he was in a small town, we might have used the virtual world to enhance the story. so as he was going through his traumatic memory we would show elements of the world that we thought would help engage him in his emotional experience so he could then go through systemically an learn that the cues to his memory were no longer dangerous in the current context back here in the united states. >> lisa, tell me something about light and imaging? >> well, remember we talked about medial prefrontal cortex being underactive in ptsd. it turns out that wth successful cognitive behavioral therapy activation in medical prefrontal cortex can actually increase. and i think that's really important. i think most people think that brain activation is hard wired and it's immutable. but actually that's not the case some so even with the behavioral or cognitive technique you can actually change brain function. the other thing that imaging has helped with in the
12:40 pm
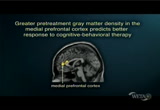
prediction of treatment response, this is a very small literature in ptsd at this point. but clinicians have known for a long time, patients have known for a long time that not everyone will respond to a given treatment so wouldn't it be nation to have an objective, maybe biological indicator of treatment response. in an individual. so some studies have started to address this using imaging. and one particular study has found that the greater the gray matter density before treatment, the better 9 response to cognitive behavioral therapy. so in a sense at least in this one study that definitely needs replication,im ageing can help predict treatment response. >> what is the link between genetics and treatment? >> sure, solisa brought up different days that biologically we can understand whether people respond differently to drugs or why they might be sensitive it turns out that as eric talked about earlier, genetic studies based on twin studies suggested that given the same trauma, about
12:41 pm

30 to 40% of the risk for who develops ptsd versus without does not is genetically mediated there are a number of genes starting to come out, one is the serotonin transporter. the serotonin transporter has been associated in a number of studies looking at stress dependency or depression and ptsd. we had study out last year showing from a campus shooting in illinois that women who had the risk alil, in this case the s verse of the serotonin transport were more likely toan develop ptsd after the same expose sheer than women who hit other vision this is a study showing that their amigdalas are hyperactivated for those that have this. another ways that genetics is helping us under be stand the neurobuy lodge is for helping us understand how the environment of trauma intersects with biology to put-- leads to differential risk. it turns out one of the higher risk factor of ptsd
12:42 pm
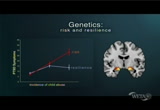
is child abuse. there are plenty that didn't have but if you have child abuse, hall treatment and abuse will you have a higher risk after adult trauma. we think it's the same sense at thisization process. this particular gene is associated with the stress hormone feedback system. and turns out one version is associate wd increased risk for adult ptsd with child abuse and the other with more resiliences and they also showed this differential gene version predicted differential amigdala response to fear again. >> this idea of the biological mechanisms for resilliance is another fascinating problem. so two people can have the same exposure but one has a genetic predisposition to is greater resilliance, can handle it better this is really quite fascinating. one can identify the factors that allow people to do it. one could really discourage people who can't handle these kinds of situations, of going into certain kinds of battle. >> the genetics show us new biological pathways to target with new drugs.
12:43 pm
>> any barriers that prevent people from seeking serious treatment? >> i think john explained well that with ptsd when people think about the trauma they feel anxious, uncomfortable. it's painful. so people just inevitably friday to avoid that. and going to seek help makes you sort of realize that there is a problem that needs attention. and then often the treatments we offer get people into a situation where they have to focus repeatedly on the trauma so people just naturally don't do it. >> the other thing as joanne was saying was also stigma, particularly in the military flchl is still a lot of stigma about seeking treatment and sort of a way of saying people are concerned that i'm back and people realistically think it may affect cat rears. that inhibits some people from getting treatment. >> so what do we do about veterans so that we can help? >> i would say there is a lot of changes taking place over the past ten years regarding ptsd in the
12:44 pm

military where the generals are standing up, jumping up and down saying you've got a problem. go see someone. get some help. and they do. they're sending all sorts of mental health teams they call them with every single unit going over to 9 war zone. >> tell me more about fear conditioning. >> you know, and how fear conditioning is a basis for a kind of basis for fear exposure therapy? >> well, as we were talking about earlier with kerry, the model is a classical conditioning model so you are learning to be-- you're learning what happens when you have ptsd, you have had a trauma. and a biological cascade of events occurred in which you perceive a threat to your life. as that threat is occurring you are encoding a whole array of sensory elements in your brain. >> also as occurs with cues that are neutral and you learn to associate the neutral clues with the threatening clues, so this is how to replicate
12:45 pm

classical conditioning. >> exactly. so going back to this stairwell. >> rose: so as we close out this, tell me about how you are today? >> well, i'm a lot better. i feel better. and but it just doesn't go away. and i went through after the dod study with joann's program there, when i moved to rhode island and went to the va. the va has a very formallized program now on treating ptsd. and just like your-- it's hard work. you have to put effort into it. and the va also gives you homework. you have to do writing, you have to write about it. and focus on one thing at a time. >> we didn't give you any homework though. >> no, you didn't. but i will go back. i'm tacking a break from it now because you can't do this stuff all the time. it's hard. >> this is an editorial on "the new york times" on december 10th. veterans of afghanistan and iraq wars have benefited from a growing, if still incomplete, understanding of
12:46 pm

post traumatic stress disorder. the government has gotten better at recognizing the affliction and giving them medical care and benefits they deserve. vietnam veterans are not always so lucky. and it goes on to talk about the lawsuit and what's come out about that. >> i read that. >> rose: do we all agree that there is increased understanding because people are now talking about it a lot more? the recognition has reached a critical mass. that this is an issue that will not go away and that we have to, the government and the private sector and friends and support groups, you know, have to come forward with the full awareness of this is pervasive and troubling. >> it is. and i think the more we talk about it, the more we literally bring it to the table here and on your show and in 9 department of defence in general, it doesn't have the stigma that it had let's say even five years ago.
12:47 pm

>> yeah. >> i think more than charlie and the rest of us talking about t you're talking about it. >> it's not even close yet. >> exactly right. because it's not just me. it's not just military either. as all of you have brought up. whether it's domestic abuse, other sorts of trauma. >> listen this, in "the new york times" article. yale stulds found that more than 250,000 vietnam era veterans, 250,000 had other than honorable discharges. and thousands probably had ptsd. but the plaintiffs are seeking seems only fair, that the military got consistent and medically approachable standards it to consider ptsd when reviewing those discharges. i want that honorable, mr. shepherd said, i did do my part. >> that's very true. >> absolutely right. >> obviously it can't exchution-- excuse criminal behavior. but never's not talking about criminal behavior. they're talking about less than honorable, which is,
12:48 pm

that could be anything. it's not really a crime. maybe you just don't fit in well. >> it is a consequence of service. >> correct. and they didn't know about ptsd back then. and they go back to george paton slapping that soldier for having combat -- >> what is painful for me and probably for kerry as well since-- is that how come the american psychiatric community did not wake up to post traumatic stress disorder until the vietnam war? why didn't they see this earlier? so the whole medical community has been slow to responding to this, realizing how important it is so a lot of people contributed to the fact that it was a late-- . >> rose: are you asking why or are you saying -- >> well, i'm saying it, yes. >> what is also ironic as you brought up earlier that i really believe is that because of this awareness of the core symptoms being in this basic emotion that is so well shared, that the chances are we're going understand the bake meck nisms of ptsd.
12:49 pm

>> much better than skits friend yap. and we have treatments coming along that are encouraging. so both the mechanism of the disease and the treatment is something we've made enormous progress with. >> let me do this. ask each of you on this particular subject what is the question that you most want to see answered? >> well, in as much as my work has been devoted to translating the science into clinical practice, i strongly believe that if a patient were to come in to our hospital we would be able to treat their ptsd and greatly improve the disabling symptoms so that they could live a fuller, more productive life. the biggest problem is getting people in our door. so i found myself becoming much more interested in the policy questions related to training specialists to developing a network of treatment around the country and specifically to what we can all do, each and every one of us about overcoming the stigma associated with mental illness in general. and with ptsd particularly, among our soldiers and
12:50 pm

warriors and cops and firefighters. >> i'm excited about the continuing convergence of animal neurobuy only and human imaging and genetics for to us really be able to understand the mechanism of how a psychiatric disorder works also. >> rose: you want to understand how it works. >> and from that we will develop treatments. >> rose: how far away is that? >> i think we're within a decade. >> dow want to say something. >> well, one of the the approaches that joanne is using in her study that grew from the animal work was a particular drug that enhances the emotional learning as you mentioned of the extinction-based therapy. and from that they were able to take it to humans and show that it enhances exposure therapy in virtual reality exposure, as one example. >> i'm really interested in being able to take the science that folks like kerry and lisa are bringing to help us understand ptsd to develop better treatments. and you know as dr. kandel pointed out ptsd is really the only disorder where we
12:51 pm

actually know when it started. we know something happened to somebody. it changed them and they are never the same. we could come figure out sort of more about those mechanisms and development treatments that would be useful early on and really be able to prevent a lot of the suffering, i think that's really where the field should be going. and i would be excited about seeing that happen. >> and along the lines that i would say, in a layman's terms would be are you ever going to get to the point with you can precondition us soldiers or anyone growing up, and i don't know if it's a cultural medical thing that you can dop. because we certainly are not hard wired to really deal with this in a much better way. and i think if we had the tools before as young people then maybe we would do bet we are it in the long run. >> i think there are probably many important questions. i guess some questions that i'm interested in are maybe
12:52 pm

identifying preexisting risk factors for ptsd or more generally. >> rose: that is fascinating. we haven't talked much about that. >> more generally biological markers that can help with diagnosis, perhaps in the future or prediction of treatment response. >> i like this last point that lisa made. we have an amazingly good understanding of post traumatic stress disorder. in part because it feeds into the biology of emotion which we understand well. but i think this is the tip of the iceberg. i don't think these three structures explained the whole sort of if you will neurocircuit of the emotional response to a stressful stimulus. and this is a disorder in which one could work this out. and would give us tremendous insight into how a psychiatric disease is really established in the brain. and since there is so much overlap, there is overlap between this disorder and panic disorder. there is overlap between this disorder and drug addiction. so if we get profound insight into this disease it will help us understanding other psychiatric diseases.
12:53 pm
>> is this of all the things, the many things that we have studied on this program, all the episodes that we have gone through over two years, one of those cases where cognitive therapy can play a significant role? >> absolutely. cognitive therapy has been a revolution psychotherapy because it brought a different approach, not insight but understanding cognitive style. and two erin beck from the very begin asking outcome studies. he didn't just say i know the patient is getting better because i sense he's getting better. this is better than placebo, it's better than selective serotonin outtake inhibitors to show solid evidence this is why cognitive behavior therapy is reimbursed in the british health-care system why many of the forms of therapy are not. >> but not here? >> here it's vaguer. >> not so well. >> not so well, yeah. >> rose: so next time we are going to sum up science and government, huh? >> you'll handle government, i'll try to handle science. >> tell the audience about -- >> i think the impact of
12:54 pm

neuroscience on public policy is enormous. witnesses in court, how reliable is their testimony. what have we learned can predict outcome. delay of gratification, other kinds of things like this. how reliable is intuitive judgement. many things that have come out of neurobiology that affected public policy and will have have a good time discussing it. >> rose: all that very much. >> thanks so much. >> rose: thank you thank you for joining us as we continue our look into the remarkable organ, the brain, and not just how functional it can be, but also what happens when there is dysfunction and what we are learning from dysfunction in order to more carefully and productively engage treatments. thank you for joining us. >>e you next time.
12:55 pm

orunrlunngrlha cry rose has been provided ha t the coca-cola company, supporting this program coca-cola company, supporting this program since 2 o



12:59 pm
>> i'm ric edelman. on today's show, how a destination wedding can save you money. what financial advisors are saying about gold, and a conversation with b.e.t.'s bob johnson. all that, and more, on this edition of "the truth about money."
136 Views
IN COLLECTIONS
WETA (PBS) Television Archive
Television Archive  Television Archive News Search Service
Television Archive News Search Service 
Uploaded by TV Archive on
